What are the Changes to OASIS E?
We keep saying it, the only constant is change. With CMS, if something stayed the same for too long, we'd worry. In 2023, CMS will begin to use OASIS E. We wrote about how many new items there were on OASIS E. You can read that here. In this blog, we'll highlight some of the new items and go a little more in depth with some of them. There's a few new ones and some really new concepts from previous versions of OASIS. There will certainly be a learning curve to understand some of the new items.
We always urge readers to use us as a resource and not THE source for OASIS. CMS has a lot of great information about OASIS E. Here are some helpful links for OASIS. OASIS E PDF OASIS E Guidance Manual One of our most popular articles is called OASIS Documentation for Dummies. You can read that here.
OASIS E Changes
CMS uses OASIS data to track certain data. Remember, OASIS stands for Outcome and Assessment Information Set. Literally, we're providing CMS (Medicare and Medicaid) with information so it can best administer its programs. Therefore, it is imperative that we provide the most accurate information possible so that CMS has the best chance to make the best policies and decisions. We always say "Data drives decisions. Good Data Drives Great Decisions." It is especially important here.
OASIS E has several new items. 27 to be exact. However, many of the changes are simply removing an older question and replacing it with either one or more related questions but getting more information, or highlight interest in a different area. A perfect example of this is on M1040 (Race/Ethnicity). This question is removed in OASIS E, but replaced with three new questions and a 4th closely related. Those are A1005 (Ethnicity), A1010 (Race), and A1110 (Language). A1250 (Transportation) is also new. This is looking to see how transportation has impacted a patient's ability to receive care. Per OASIS Guidance Manual A1250 "Access to transportation for ongoing health care and medication access needs is essential to effective care management. Understanding patient transportation needs can help organizations assess barriers to care and facilitate connections with available community resources."
A2120-A2124 Med Profile Provision to Provider/Patient
Ensuring Continuity of care is essential. These new items are related. CMS wants to ensure that reconciled medication lists are provided to the subsequent provider (because of discharge or transfer) and the patient (or family). Also, important is understanding HOW this was done. Special note: If a patient is not taking medication, this must be documented, but coded as 1.
B0200- Hearing
This is a new question. CMS has asked about Vision for some time, it is only rational to think that collecting hearing data is equally important to determine safety in the home. Also, many patients can pretend to hear and understand instruction and teaching. Documenting hearing status will be helpful and paint a more accurate picture of the patient. Specific guidance from CMS regarding patients who may have cognitive impairment or other issues. "Patients who are unable to respond to a standard hearing assessment due to cognitive impairment will require alternate assessment methods. The patient can be observed in their normal environment. Do they respond (e.g., turn their head) when a noise is made at a normal level? Does the patient seem to respond only to specific noise in a quiet environment? Assess whether the patient responds only to loud noise or do they not respond at all."
B1000 Vision
CMS removed M1200 from OASIS D1. CMS is still interested in that information. M1200 only allowed for 3 responses. Now, B1000 allows for 5 responses. Also, B1000 mentions the ability to see in adequate light. One thing to think about is if the patient lives in a place with adequate light at all. Many patients live in older homes or apartments without many lights or windows. Further, M1200 had three choices. B1000 now has 5. This will give more accurate information. From the guidance manual: "Some patients have never learned to read or are unable to read English. In such cases, ask the patient to read numbers, such as dates or page numbers, or to name items in small pictures. Be sure to display this information in two sizes (equivalent to regular and large print)."
B1300 Health Literacy
This is a new question. We believe it is also very helpful because many people don't speak medical terminology. It can be easy to assume that the patient same level of knowledge and training as our clinicians. We can speak fast that makes things over their head. I have to regularly go help a friend of mine read and understand medications, medical instructions, and sometimes even explain what the definition of a problem they're having is. Some doctors don't spend adequate time explaining, or perhaps a patient may have forgot what the doctor said. I know I have. CMS says "Poor health literacy is linked to lower levels of knowledge of health, worse outcomes, and the receipt of fewer preventive services, higher medical costs and rates of emergency department use." Be aware that cognitive function should be taken into consideration for this question.
Section C: Cognitive Patterns
There are several new questions in this section. This will require quite a bit of education and practice for clinicians to know and understand this section well.
What is BIMS in Home Health?
C0100- Should Brief Interview for Mental Status (BIMS) be Conducted?
This seems self-explanatory. BIMS stands for Brief Interview for Mental Status. This is a structured cognitive interview. CMS says, "A structured cognitive test is more accurate and reliable than observation alone for observing cognitive performance." This question determines if a BIMS should be conducted. Most people should have an interview. If the response is response 0 (No), then skip the BIMS items. This response should be "if the interview should not be conducted because the patient is rarely/never understood; cannot respond verbally, in writing, or using another method; or an interpreter is needed but not available." The BIMS should be attempted for all patients per CMS.
C0200-C0500 Brief Interview for Mental Status (BIMS)
The clinician should wait about 30 seconds for a response. Some responses may be nonsensical. The guidance manual is very helpful to understand the BIMS. That can be found in Section C. Clinicians should read through this to be familiar with the process. There are contingencies to do the BIMS in written form as well.
C0200- Repetition of Three Words
This section details how the interview should be handled. It also is very clear that it shouldn't be changed. Use the same approach, as outlined, every time. This makes for more consistent score and assessment. The interview is conducted by having the clinician say "I am going to say three words for you to remember. Please repeat the words after I have said all three. The words are: Sock, blue, and bed. Now tell me those three words." The clinician then records the number of words repeated after the first attempt. (0,1,2,3) After the first attempt repeat the words using cues "sock, something to wear; blue, a color; bed, a piece of furniture. The clinician may repeat the words up to two more times.
C0300 - Temporal Orientation this is to determine orientation to year, month, and day.
The clinician will say "Please tell me what year it is right now." The answers are from 0-3. 0 is off by 5 or more years, 1 is missed by 2-5 years, 2 is missed by 1 year, and 3 is correct. The clinician will then ask "What month are we in right now?" the available responses are: 0-2. 0 means missed by greater than 1 month. 1 is Missed by 6 days to 1 month, 2 is Accurate within 5 days. The clinician will then ask "What day of the week is today?" 0, is incorrect or no answer, and 1 is correct.
C0400- Recall
The clinician will ask the patient "Let's go back to an earlier question. What were those three words that I asked you to repeat?" If the patient is unable the patient will give a clue, something to wear, a color, a piece of furniture. part A: is patient able to recall sock, 0-2. 0 unable to recall, 1- Yes, able to recall with cue, 2- Yes, no clue required. This is repeated with the words blue and bed. The clue or approach is the same with or without prompts.
C0500- BIMS Summary Score
The clinician will total up the scores from the previous 4 questions. If a patient refuses to answer, the clinician should mark the answer as incorrect. "The BIMS total score is highly correlated with Mini-Mental State Exam (MMSE; Folstein, Folstein, & McHugh, 1975) scores. Scores from a carefully conducted BIMS assessment where patients can hear all questions and the patient is not delirious suggest the following distributions:
Section D Mood
M1730 has been removed and replaced with a more thorough screening on mood.
D0150 Patient Mood Interview
This section and interview is a little technical. Rather than explain each one, we have put an image from the OASIS form below. Remember, Column 1 represents if system is present in the last 2 weeks (0- No- also enter 0 in column 2), 1 - Yes- (enter 0-3 in column 2), or 9 no Response- leave column 2 blank. If the response in column 2 for questions A or B is 2 or 3, then the clinician proceeds with asking questions C-I. The responses in Column 2 should be 0,1,2,3 with 0 being never or 1 day, 1 (2-6 days), 2 (7-11 or half or more of the days), 3 (12-14 days)
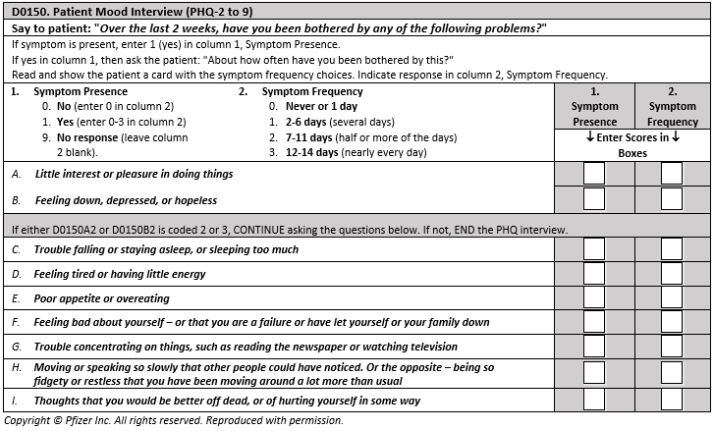
Mental health is becoming more and more important and recognized. Social isolation among the senior population can and does have a negative impact on overall health and wellbeing. This does NOT indicate a diagnosis of depression. Only doctors can diagnose. But these are indicators that should be followed up on with a doctor if the overall score is high. As in a lot of things, context is key. By properly introducing the interview, clinicians can get better answers and accuracy. Here's an example “I am going to ask you some questions about your mood and feelings over the past 2 weeks. I will also ask about some common problems that are known to go along with feeling down. Some of the questions might seem personal, but everyone is asked to answer them. This will help us provide you with better care.” Also, these shouldn't be asked differently or defined. These are interpreted by the patient as to what the meanings are. Here's a tip from CMS: "Noncommittal responses such as “not really” should be explored. Patients may be reluctant to report symptoms and should be gently encouraged to tell you if the symptom bothered them, even if it was only some of the time. This is known as probing. Probe by asking neutral or nondirective questions such as:
D0160- Total Severity Score
The clinician will then add up all the responses from column 2 into a total score. This can be tracked over time and is important for determining mental health or change in mental health status. In addition, PHQ-2 to 9 Total Severity Score can be used to track changes in severity over time.
Total Severity Score can be interpreted as follows:
D0700 Social Isolation
The clinician asks how often the patient feels lonely or isolated from those around them. This is looking to determine "the patient’s actual or perceived lack of contact with other people, such as living alone or residing in a remote area." There 9 options (0-8) for this. This should be a patient self-report response.
Section J
M1242 has been removed from OASIS. This question has been replaced by 3 other questions- seeking more clarity and specificity with pain. These questions are J0510 (Pain effect on sleep), J0520 (Pain interference with therapy), and J0530 (Pain interfering with activity)
These questions are determining how pain affects the life of the patient. Again, this has to do in the last 5 days. There is a new part to J0510, the response of 0 "Does not apply No pain experienced in the last 5 days." If this response is given, then the clinician skips to M1400. CMS guidance says "The key difference between code 0, Does not apply and code 1, Rarely or not at all is that for code 0, the patient reports no pain/hurting in the past 5 days, and code 1, the patient reports pain/hurting HAS been present in the past 5 days, but has rarely or not at all impacted sleep." This is repeated for the next two questions.
K0520- Nutritional Approaches
This section reviews all the nutritional approaches from admission to discharge for a patient. There are several options. Note: IV feeding is only to be marked if used for nutrition or hydration and not for delivery of medication or flushing.
N0415- High Risk Drug Classes: Use and Indication
This identifies if the patient is taking any prescribed medications in specific drug classes and whether the indication was noted for all medications in that drug class. The guidebook says "Patients who take medications in these high-risk drug classes are at risk for side effects that can adversely affect health, safety, and quality of life."
O0110- Special Treatments, Procedures, and Programs
This is pretty straightforward. These items can have a profound effect on patient health status, self-image, dignity, and quality of life. These are looking if the patient has treatments and how the treatments are administered. Chemotherapy, Oxygen Therapy, Suctioning, Tracheostomy Care, Invasive Medical Ventilator, Non-Invasive Medical Ventilator (BiPAP or CPAP), IV Medications, Transfusions, Dialysis, IV Access, or none of the above.
Conclusion
Phew! That was pretty long. Home Care Answers wants to be on the leading edge of training and information. This helps agencies and clinicians know what is new so that the patient receives the best care possible, AND that CMS receives the most accurate information to determine future policy. We'd love to help any agency see how they're doing. Click here for us to review charts at no cost to you.