
What is HHVBP? What is Home Health Value Based Purchasing?
The only thing constant is change. In 2023, CMS really outdid themselves. CMS is introducing OASIS E (read about OASIS E updates here) AND starting HHVBP. HHVBP means Home Health Value Based Purchasing. In lay terms, it means that CMS wants home health agencies to improve outcomes and quality of care without spending more money. There's a bit of a back story on this, and it is helpful to understand where CMS is coming from in rolling this out. Originally, CMS launched Home Health Value Based Purchasing (HHVBP) in 2016 in 9 states. The aim was to try to incentivize agencies with higher reimbursement rates if agencies (HHAs) could provide higher quality care and outcomes, keep patients out of the hospital, and provide a good experience. That's exactly what happened. Agencies in those 9 states increased Total Performance Scores by 4.6% and saved Medicare $141 million without evidence of adverse risks. This seemed to be a win for all involved. Basically, HHVBP means that if agencies can provide better service compared to their peers, they can get more reimbursement. If the quality is less compared to peers, then they get less reimbursement. If it is average compared to peers, then it remains basically the same.
In 2021, it was announced that the pilot program of HHVBP would end and all agencies in the US would begin roll out of HHVBP starting 2022. 2022 is a data gathering year for all agencies. Starting in 2023 (this is called Performance Year One), the information that HHAs provide through various measures and statistics will impact payment in 2025 (called CY 2025 Payment Year One). So, it's REALLY important to start to pay attention and get it right. CMS will pay an increase of up to 5% or a decrease of up to 5% to agencies compared against agencies of like size across the country. These payments will track 2 years later. So, 2023 data will have payment adjusted in 2025, data from 2024 will have payment adjusted in 2026, etc.
Repeat after me: IT IS STILL ALL ABOUT THE PATIENT! Too often, agencies aren't getting credit for the good work they're doing because of OASIS inaccuracies which fail to capture the actual improvement that is clearly happening. To review our OASIS for dummies blog post, click here.
HHVBP Model Expansion 101
HHVBP is pretty complicated. We'll try to give a high-level view of HHVBP and key components of the program. For a comprehensive explanation, CMS has given a lot of resources to prepare. Here are some links for reference. HHVBP Model Guide, HHVBP FAQs, 2022 CMS Final Rule for Home Health, HHVBP CMS Resources. We've read through these (and more) to try to help agencies understand HHVBP better and better prepare for implementation. A successful implementation can mean an increase of up to 5% in reimbursement. At a bare minimum, it would behoove agencies to be prepared enough to avoid having a 5% reduction in reimbursement.
2022 is what is called a Pre-Implementation Year. This is a trial run- use the information provided to learn and be ready for when CMS starts counting- CY 2023. This is when CMS starts to calculate the Home Health Agency Total Performance Score (TPS).
What Payer Sources Contribute for HHVBP?
This is an area where agencies need to pay attention. Agencies can be very tempted to not pay much attention on OASIS to Medicaid payer sources since OASIS and coding don't make a financial difference. It matters greatly now. Agencies would do well to pay attention to all OASIS given HHVBP is using all CMS associated payer sources. These are Medicare FFS, Medicare Advantage, Medicaid FFS, Medicaid Managed Care. For claims based measures, Medicare FFS are what is tracked. Here's
HHVBP- What makes a TPS?
CMS is using data that is already being provided by HHAs to calculate TPS- therefore agencies DO NOT need to provide additional data for HHVBP. That's a sort of win for agencies. They are already submitting that data for HH QRP.
There are 3 parts to the TPS for an agency. There are OASIS Based, Claims Based, and HHCAHPS Survey Based components. Further, Agencies must have at least 20 home health quality episodes for OASIS and Claims Based Measures, and 40 completed surveys for HHCAHPS information. There must be at least 5 of the 12 components available to be able to calculate a score. Is your head spinning yet?
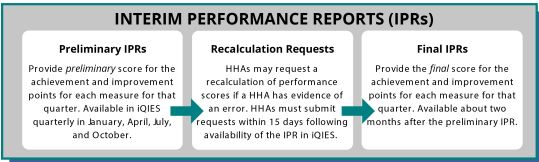
There will reports that are developed based off the information provided by agencies from claims. These are called Interim Performance Reports (IPR). Agencies review these reports as the preliminary report, and can actually ask CMS (or intermediary) to recalculate certain claims where there is evidence of an error. Agencies have 15 days to file recalculation requests from the time the HHA receives the IPR. After the preliminary and recalculation request, the final IPR is posted- about 2 months after the preliminary IPR. Here is what the flow looks like below:
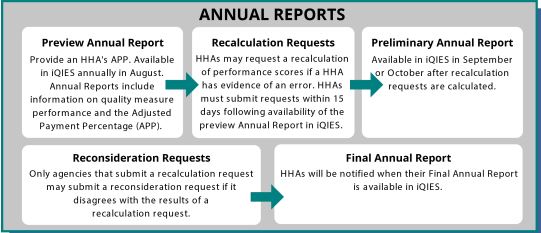
Agencies then will receive annual reports that will have 5 steps to it. This process will be similar to the IPR process. The annual reports will be available in August. There will be a preview of the annual report- which sets the Adjusted Payment Percentage (APP) for the following year This will be an increase or decrease of up to 5% based on comparisons of comparable agencies. followed by recalculation requests if there is evidence of an error. Again, this must be submitted within 15 days of receipt of the preliminary annual report found in iQIES. There is the preliminary annual report available around September or October. There is a reconsideration request stage only for agencies who filed recalculation requests and if the agency disagrees with the results of the recalculation request. After that, agencies will be notified when the final report available in iQIES.
Here's what the final report process looks like below:
What are the Quality Measures in HHVBP?
There are five parts to Quality Measures in HHVBP. There are three stand alone OASIS questions, these are M1400 (Improvement in Dyspnea), M2420 (Discharge to Community), and M2020 (Oral Medications). The next two are a composite score of several ADL and IADLS: Change in Self Care and Change in Mobility. The OASIS questions that deal with Change in Self Care are M1800 (Grooming), M1810 (Upper Body Dressing), M1820 (Lower Body Dressing), M1830 (Bathing), M1845(Toileting Hygiene), and M1870 (Eating). The OASIS questions that deal with change in mobility are M1840 (Toilet Transferring), M1850 (Bed Transferring), and M1860 (Ambulation/Locomotion).
The ADL/IADL questions for Self Care and Mobility are added together to generate a Total Normalized Composite score. Per CMS "The Home Health Value-Based Purchasing (HHVBP) composite measures, Total Normalized Composite (TNC) Change in Self-Care and TNC Change in Mobility, capture the magnitude of change (not just improvement) in multiple OASIS items. Therefore, they reward efforts to improve patients who are less independent at start or resumption of care, as these patients have a greater opportunity for higher TNC measure scores. Normalization accounts for the variation in the number of response options on the applicable OASIS items for each TNC Measure." Computing HHVBP Measures
Here's the process of computing the TNC from a graphic from CMS:
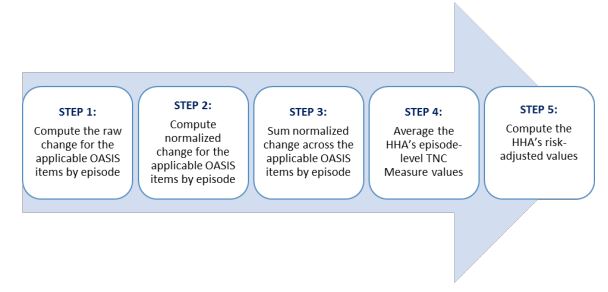
Step 1: Compute the Raw change for the applicable OASIS items by episode
Step 2: Compute Normalized change for the applicable OASIS items by episode
Step 3: Sum normalized change across the applicable OASIS items by episode
Step 4: Average the HHA's episode level TNC Measure values
Step 5: Compute the HHA's risk adjusted values
This action is much easier shown that explained. The graphic below illustrates the process better.
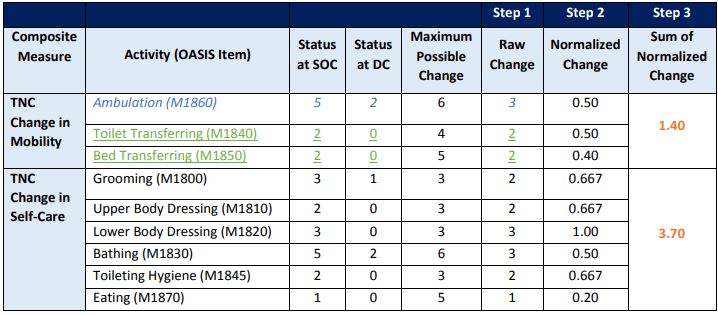
CMS recognizes that several OASIS items have more maximum possible changes than others. So, a raw change could skew the calculation one way or the other. Therefore, we must normalize the change to come up with a smoother and more consistent score. For example, on M1860, there are 6 possible changes. So if someone went from a 6 to a 0, that would be a huge score, whereas on M1840, if someone went from a 4 to a 0, that is still significant, but the maximum raw score would still be less than M1860- thereby impacting the calculation. To remedy that, the calculation to normalize a change then takes the raw change score and divides it by the maximum possible change to get a normalized change. The totals are then added up to get a sum of a normalized change.
A special note from CMS is important to understand. "Please note that patients who are fully independent at start or resumption of care ARE included in the calculations. Patients who are fully independent can either remain the same or worsen. If the patient worsens, the episode will earn a negative change score." Many clinicians score patients as independent regardless of the condition or fail to take into account the overall condition of the patient compared to himself or herself. For example, if someone is blind, and can ambulate, the clinician may be tempted to score the patient as independent. However, compared to a non-blind person or the same patient with full vision, the patient is not able to ambulate independently. Therefore, it would be inaccurate to score that patient as independent.
Step 4 then takes the sums of all of the patients and averages the total normalized composite to adjust for anomalies.
Step 5 then takes observed and predicted scores to get a risk adjusted score.
It is important to note that these measures are measured against Start of Care or Resumption of Care and discharge. Discharge OASIS have long been an afterthought for agencies. Star ratings are impacted by SOC and Discharge, but there weren't financial implications, until now. Having a trained eye that is looking at the SOC, ROC, and Discharge and comparing for progress is very important. This is where consistency of review and assessment becomes essential.
Further, there will be many programs that will calculate this information for you. However, knowing what goes into the scores is always helpful. We say that data drives decisions. Great data drives great decisions. Knowing how and why things happen is very important.
What Claims Based Measures are part of HHVBP?
There are two parts to this question. The first is Acute Care Hospitalizations During the First Sixty Days of Home Health Use (ACH)and Emergency Department Use Without Hospitalization During the First Sixty Days of Home Health (ED Use). The goal of HHVBP is to keep people out of the hospital and ER. Home is the best and most cost-effective place for people to heal. That has been shown time and time again. Agencies need to be aware of, and mitigate, risks for hospitalization and ED use. Some of the main causes for hospitalization are falls and infection. It could be argued that infections can cause more falls. Having proactive plans to manage infection and reduce fall risk will be essential for HHAs to mitigate hospitalization and ED use. To be sure, some patients will require hospitalization and have to go to the ER. Agencies who proactively mitigate will be more successful.
What are the HHCAHPS Measures for HHVBP?
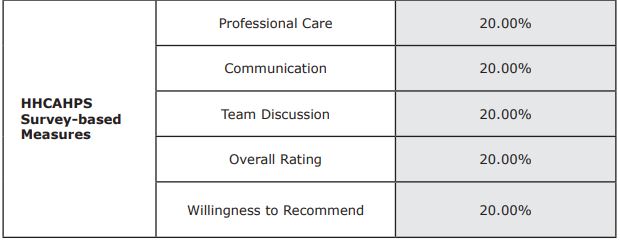
We'll not spend a lot of time on these items. From CMS "The Home Health Care Consumer Assessment of Healthcare Providers and Systems (HHCAHPS) survey is the first national standardized and publicly reported survey of home health care patients’ perspectives of their skilled home care. The HHCAHPS survey specifically presents home health patients with a set of standardized questions about their home health care providers and about the quality of their home health care. The HHCAHPS survey-based measures in the expanded HHVBP Model measure set are the following five (5) components of the survey:
How is Total Performance Score Calculated?
Below is an illustration on how TPS is calculated- per CMS explanation.
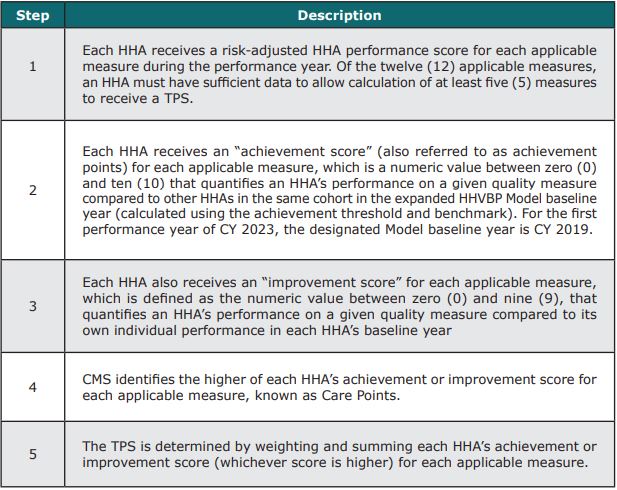
There are a lot of ways to illustrate calculating the TPS for an agency. Not every agency will have scores evenly. CMS accounted for that by putting in minimum applicable episodes and minimum thresholds. Per CMS "Minimum Number of Applicable Measures and Minimum Thresholds The calculation of a TPS requires an HHA to have sufficient measure data. The following is the minimum threshold of data an HHA must have for each applicable measure to receive a measure score:
• For OASIS-based measures, twenty (20) home health quality episodes per reporting period.
• For claims-based measures, twenty (20) home health stays per reporting period.
• For the HHCAHPS survey-based measures, forty (40) completed surveys per reporting period.
In addition, an HHA must have sufficient data to allow calculation of at least five (5) of the twelve (12) measures to receive a TPS and be eligible for a payment adjustment. A deeper explanation of TPS scoring for achievement score and improvement score and care points. It isn't easily explained. But can be viewed in this link on pages 21-26 TPS Scoring Demonstration
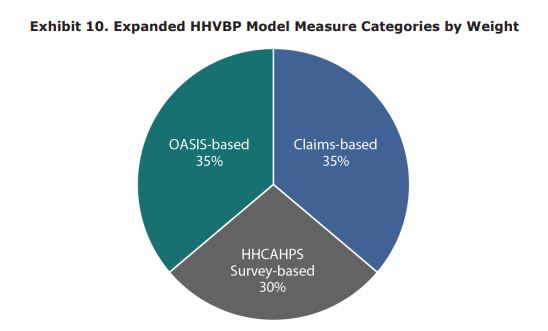
Weighting HHVBP
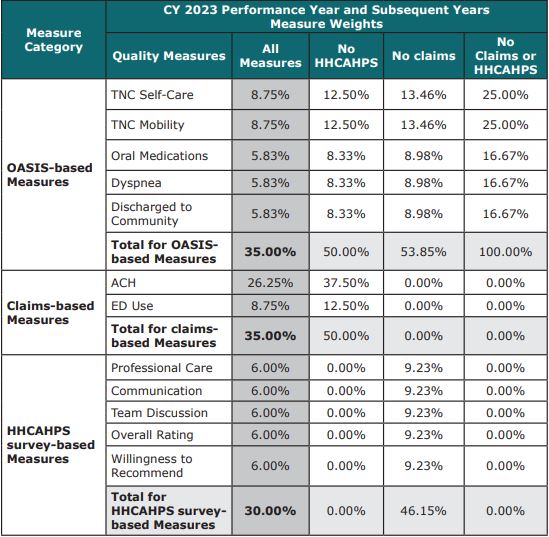
CMS weighs each portion of the measures differently. Below are some illustrations from CMS that show how each section and then each component of each measure are weighed, and re-weighed.
Overall Weights
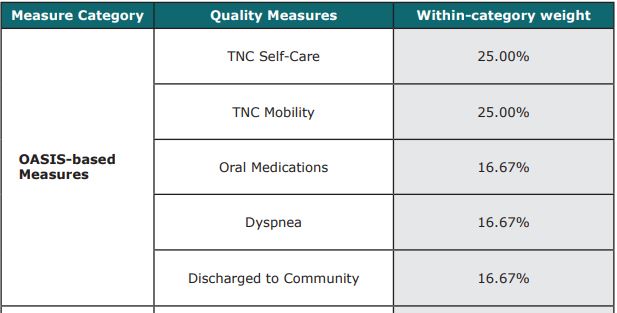
OASIS based Measures
Claims Based Measures

HHCAHPS Measures
CMS has accounted for every scenario in developing HHVBP. No agency will have all of the measures needed to score perfectly. Below is a great illustration from CMS that shows the individual contribution weighting broken by OASIS question and then reweighting scenarios if certain criteria aren't met.
Conclusion

Does your head hurt? HHVBP can be daunting and overwhelming. It can be very beneficial to agencies for those who perform well. Many things aren't necessarily in the agencies control, but the agency does control the OASIS process. Home Care Answers is dedicated to helping our agency partners achieve the most accurate OASIS possible. Accuracy brings increased revenue, improved outcomes (you get the credit you deserve for the good work you're doing but aren't being recognized for), improved star ratings, and now improved HHVBP scoring. By letting us help you with OASIS at the beginning AND at discharge, you can be assured that your OASIS scoring will be accurate and then let the chips fall where they may.