
What is Discharge Function Score (DC Function)?
Home Health hasn't had much of a breather the last few years between PDGM and HHVBP implementation, oh and a pandemic. And Inflation. And Retention. And Staffing issues. And growing expenses. And continual CMS headaches with reimbursement. And Medicare Advantage (disadvantage- did I say that out loud?) It's a lot to keep up with. It's not always easy or pleasant. With all of the changes, it's sometimes like taking a drink from a firehose. You get drenched, but not quenched.
For 2025, CMS has announced changed to the Home Health Value Based Purchasing OASIS measures. You can learn more about HHVBP in a previous post (here). We're going to discuss some of the upcoming changes starting in 2025 for HHVBP. We first need to discuss some of the changes to HHVBP so we can better understand Discharge Function Score (DC Function).
What are the changes to Home Health Value Based Purchasing?
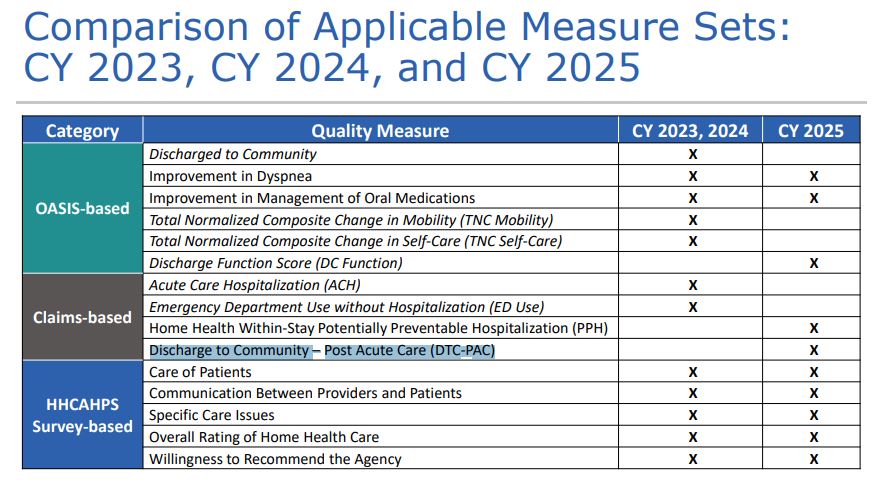
CMS had several OASIS based measures that were being tracked on HHVBP in 2023 and 2024. If you remember, CMS was tracking TNP Score on Mobility (M1860, M1840, M1850) and Self Care (Grooming M1800, Upper Body Dressing M1810, Lower Body Dressing (M1820), Bathing (M1830), Toileting Hygiene (M1845), and Eating (M1870). These measurements created a balanced score for these items called a TNC (Total Normalized Composite). These are being replaced with a Discharge Function Score (DC Function) that are based on GG Questions. We'll describe them in further detail below.
CMS is also doing away with measuring Discharge to Community measure as that wasn't a very good measurement frankly. If you want a detailed analysis on the reasoning behind these changes, you can read about them here
For Claims based measures, CMS is no longer tracking Acute Care Hospitalization and Emergency Department use without hospitalization. Those are being replaced by Home Health Within-Stay Potentially Preventable Hospitalization (PPH) and Discharge to Community – Post Acute Care (DTC-PAC). These are based off the claim and so there's not much that can be done to improve accuracy of data on that. Things happened or they didn't. The whole goal is to keep people out of the hospital by providing quality care up front in the home.
Here's a nice graphic from CMS that details what is staying and what is going. Here's the link from where the graphics came from: CMS Presentation on HHVBP Changes
What do GG questions have to do with HHVBP (Home Health Value Based Purchasing)?
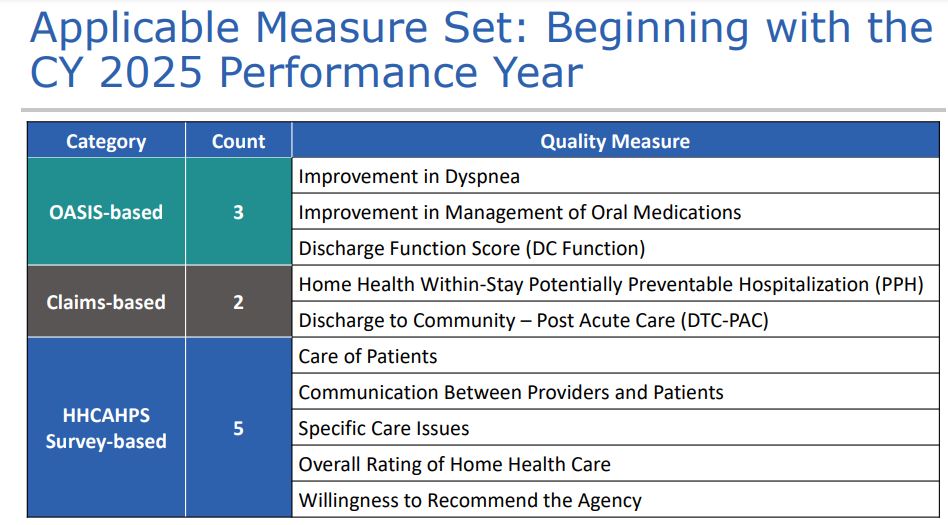
Now that we have established what is going away for HHVBP, we need to understand what will be replacing it. ADL Questions are now not part of the calculation. GG Questions will make up the DC Function Score.
GG Self Care and GG Mobility will make up the Discharge Function Score. Here is the calculation below 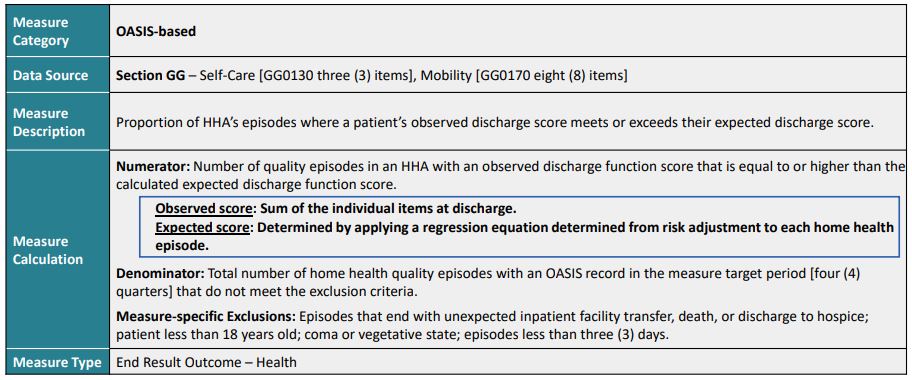
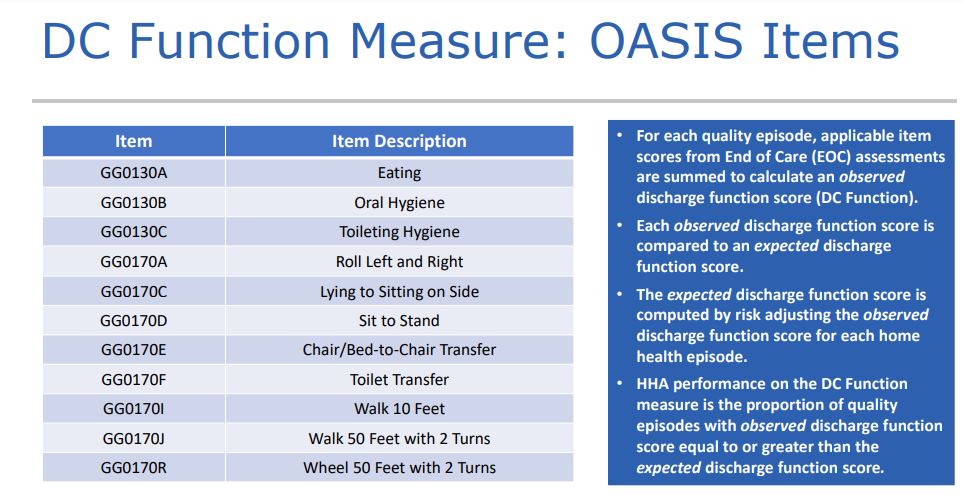
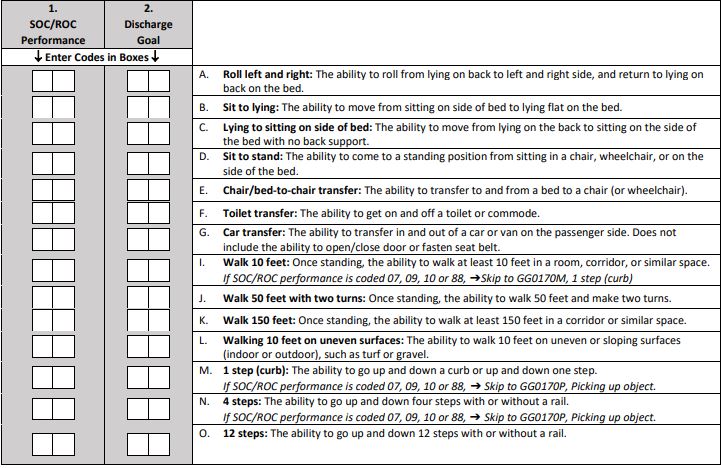
What this says is that the observed score will be divided by a risk adjusted regression of the expected score. Basically, it's saying how the patient is doing compared to how they are expected to do with a regression analysis equation. Since the regression analysis equation is fairly complicated, what needs to be focused on is having the correct scoring from the observed score. Here are the specific GG Questions that are being measured below
How do GG Questions impact HHVBP?
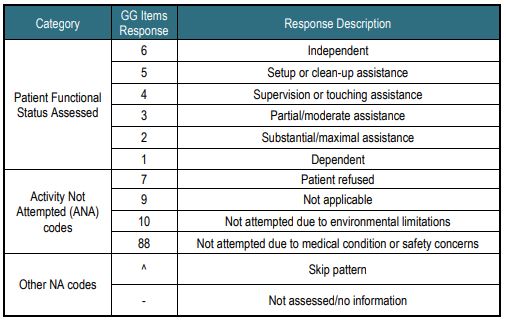
Since GG questions have been implemented, many clinicians haven't treated them seriously. They're counterintuitive from ADLs, meaning the responses are inverted. For ADLs, the lower the response (0 or 1) the more independent a patient was. In GG Questions, the lower the number, the more dependent the patient is. See below
Much has been said about the SOC and GG questions. Discharge is now becoming more important. Notice there are multiple opportunities for GG questions to be adjusted. There is the SOC/ROC OASIS where there's the GG SOC and the Discharge Goal.
Then there is the follow up scoring as above. Then upon discharge, GG Questions are assessed again. If the clinician doesn't pay much attention to the GG questions and shows that the patient is mostly independent because it is easier, but ADL questions (where payment is determined) show more dependence there is a discrepancy. Why the discrepancy? Does the clinician understand the connection between the two? Does the clinician only place value on the ADL because money is attached? Did the clinician just put answers in for GGs and not really attempt all of the tasks? If the clinician didn't put much effort into the SOC and shows the patient is more independent than the documentation and diagnoses show, how can the patient show the improvement that is likely happening? If the patient doesn't improve, then the discharge function score is compromised and the sends faulty data to CMS, HHVBP discharge function scoring is incorrect, the expected score is incorrect, which can impact the HHVBP overall TPS (Total Performance Score). If the clinician doesn't understand the question at SOC, it stands to reason that the clinician will likely be incorrect upon discharge (Or have no room for improvement upon discharge because of initial inaccuracy).
It's only the GG's will not cut it any more.
Many coding agencies skip over the GG questions. They don't even look at them. Home Care Answers does a full OASIS review, because we're after accuracy. Revenue, compliance, star ratings, and now Value Based Purchasing follows accuracy. Why would you risk not having a full review, or a company that offers partial review? Why would agencies try to skimp on such important services? I have often heard, "if it matters, pay for it." Or "buy once, cry once." Paying for quality may seem painful, but how long will an organization continue to pay in terms of lost revenue, denials, HHVBP, time, effort, and training? There is opportunity cost also. Home Care Answers can quantify the opportunity cost, compare it to its peers, and show the difference between the two, AND show agencies where they are missing on any OASIS question- from the multi state corporate level all the way to the clinician in a single branch. It's essential we get this right.