
What are the changes to Home Health Value Based Purchasing?
We've had a lot of new buzzwords in home health lately. PDGM, Value Based Purchasing, TPE, RCD, etc. There have been a lot. It hasn't been a slow drip; it's been a fire hose. Nonstop changes. Nonstop challenges. More things to add. More things to track. More things to do.
Home Health Value Based Purchasing (HHVBP) will continue to be a big buzzword in home health for the foreseeable future? Why? Because creating quality outcomes, keeping people out of the hospital, and helping patients heal in their home is a lot less expensive on CMS than sending them to the hospital or a Skilled Nursing Facility (SNF). Incentivizing home health agencies to have higher quality outcomes by giving (or taking) up to 5% of reimbursement should still cost CMS less than additional hospitalizations and SNF admits.
We've written extensively about Home Health Value Based Purchasing previously. You can catch up on them here and here. We've introduced a separate change about Discharge Function Score.
We'll discuss some of the other changes ti HHVBP in this blog in addition to touching on Discharge Function Score.
Here are the changes to VBP from a high level. CMS gave an excellent recap of the changes to HHVBP that you can find here.
If you can remember, TNC was pretty complicated. CMS seems to be making an effort to make it a little less complicated, emphasis on a little.
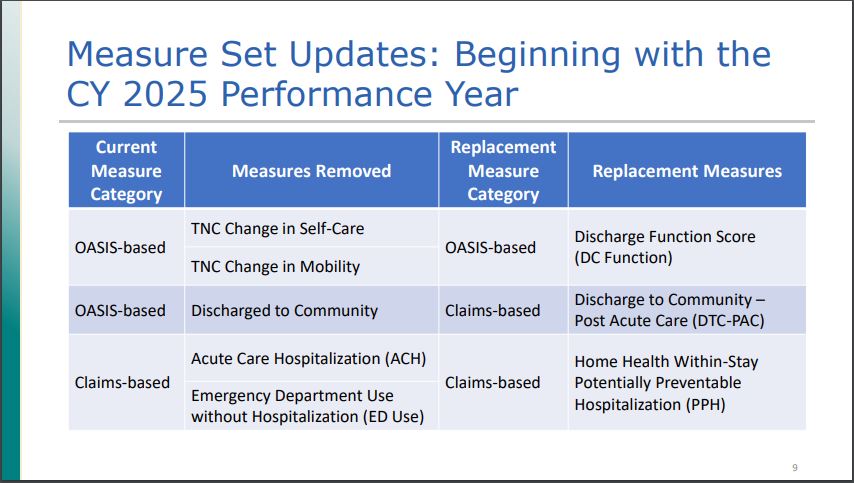
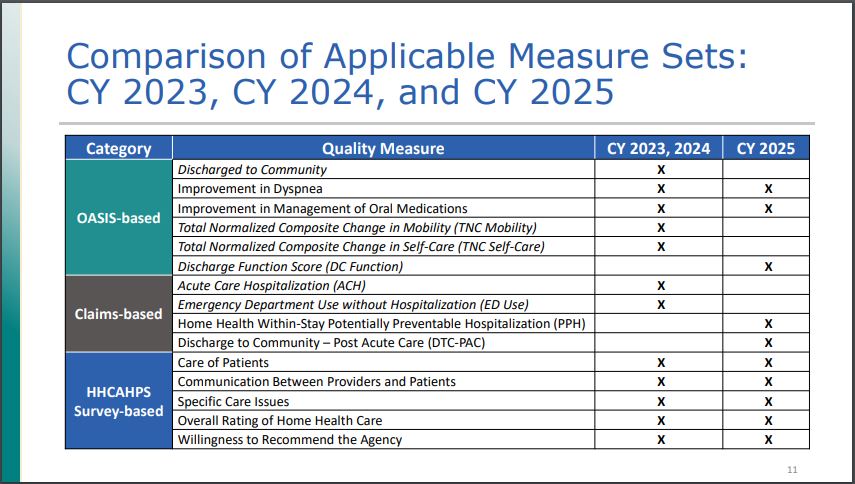
So, TNC (Total Normalized Composite Change) goes away. It will be replaced by Discharge Function score. TNC focused on the M1800 questions in OASIS (OASIS E instrument found here.) Discharge Function Score focuses on GG questions- specifically GG0130A, GG0130B, GG0130C, GG0170A-F, GG0170I, GG0170J, GG0170R
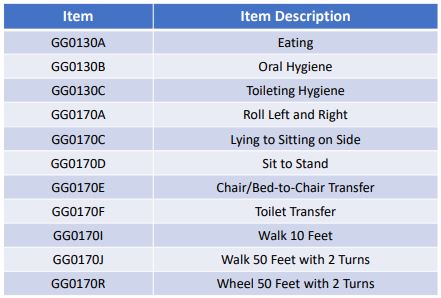
This is a pretty major shift away from the ADLs and M1800 questions to the GG questions, which are similar to M1800s, but more specific. Again, the focus is on the comparison from SOC to discharge, so getting OASIS upon SOC (or ROC) is essential so that agencies can get credit for the good work they're doing.
The Discharge Function Score is a calculation of the discharge divided by the expected discharge function score (risk adjusted regression). There's not much that can be done on the expected score, so agencies must focus on what they can control- OASIS accuracy.
Claims Based Changes
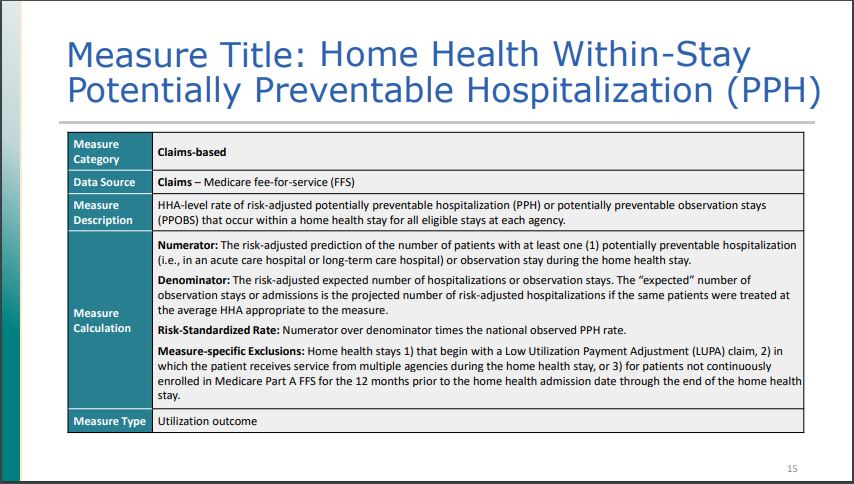
We covered the OASIS based measures above. There are changes to the claims based measures also. Previously the claims based measures were Acute Care Hospitalization and Emergency Department Use without Hospitalization (ED Use). These have been replaced by Home Health Within-Stay Potentially Preventable Hospitalization (PPH) and Discharge to Community – Post Acute Care (DTC-PAC). These are tracking the same metrics, just slightly different. For more background on Potentially Preventable Hospitalization, you can read a link here. The idea behind Potentially Preventable Hospitalization from the article were that there are 4 factors that contribute to preventable hospitalization. There are:
1) Inadequate management of chronic conditions
2) Inadequate management of infections
3) Inadequate management of other unplanned events
4) Inadequate injury prevention
If agencies are managing the above 4 things, that should, in theory, prevent a good number of patients from being readmitted to the hospital, which is exceptionally more expensive than home health care. The graphic below summarizes PPH.
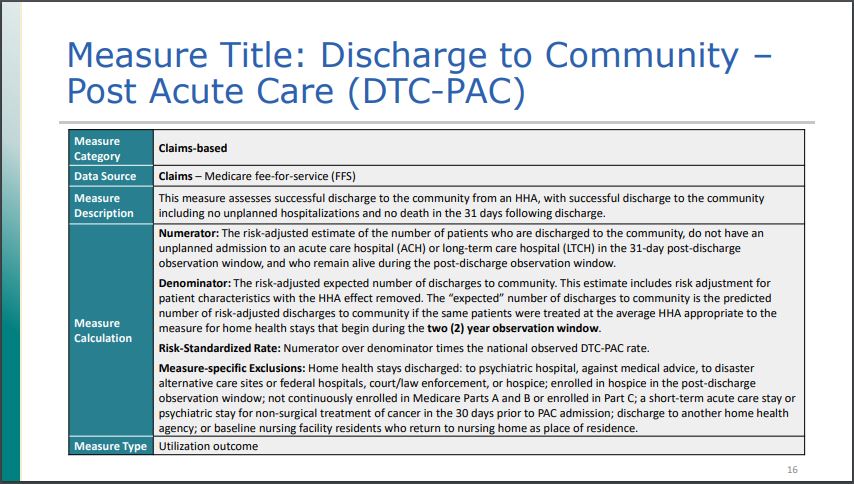
Discharge to Community- Post Acute Care
Here is a great excerpt from a Q&A about DTC-PAC and what it measures.
Q: What do the DTC-PAC measures assess?
A: The DTC-PAC measures assess successful discharge to the community from a PAC setting, with
successful discharge to the community including no unplanned rehospitalizations and no death
in the 31 days following discharge. Specifically, these measures report a provider’s riskstandardized rate of Medicare fee-for-service (FFS) patients/residents who are discharged to the
community following a PAC stay, and do not have an unplanned readmission to an acute care
hospital or LTCH in the 31 days following discharge to community, and who remain alive during
the 31 days following discharge to community. Community, for this measure, is defined as home
or self care, with or without home health services, based on Patient Discharge Status Codes 01,
06, 81, and 86 on the Medicare FFS claim. A statistical approach is used to calculate confidence
intervals for the provider’s DTC rate. These confidence intervals are then compared to the
national observed DTC rate to assign providers to performance categories for public reporting.
The performance categories are (i) better than the national rate, (ii) no different from the
national rate, and (iii) worse than the national rate. Source: CMS DTC-PAC FAQ
Again, the idea is if home health agencies can prevent patients from being readmitted (and alive) for the next 31 days, then outcomes are positive and cost CMS less than rehospitalization and readmission to hospital or Home Health, or other post acute care facility. This doesn't have much to do with OASIS accuracy as it does with quality of care and circumstances.
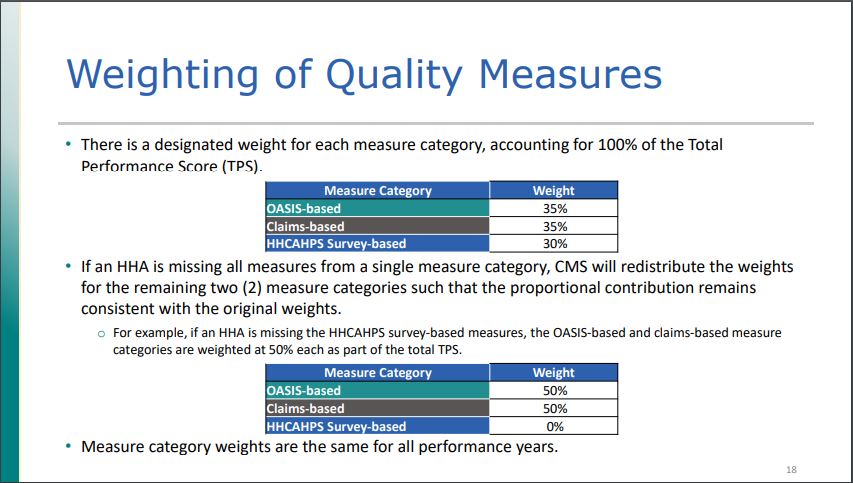
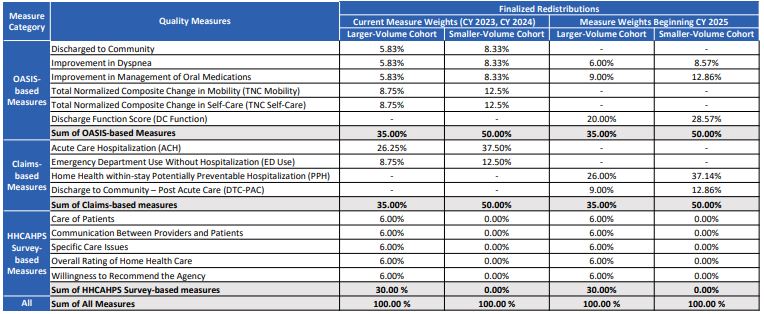
HHVBP Measure Weights
There weren't significant changes to the measure weights, so a simple graphic describing what the weights are would be most helpful.
More detail
Home Care Answers: HHVBP partner through OASIS accuracy
There are some things that agencies can control, and some they can't. Some things agencies have to manage like patient satisfaction surveys and claims based measures. But they can't necessarily control them.
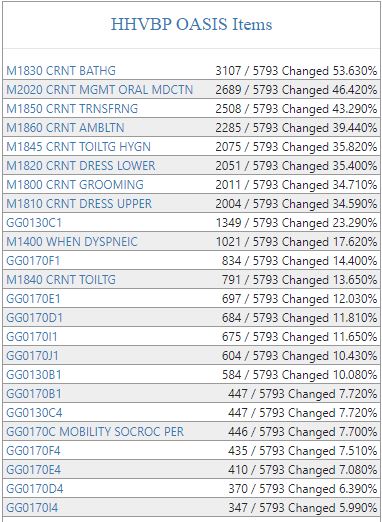
What they can control is accuracy. By getting OASIS correct at SOC, then agencies stand to have a chance at getting the outcomes upon discharge correct. If clinicians don't understand what the questions are asking, then it's difficult to get things correct from the start, and harder to get it correct (and get credit for the work you're doing) which leads to the best chance for outcomes. Home Care Answers tracks HHVBP OASIS items currently and future ones so agencies can be proactive in their efforts. By tracking SOC and then to Discharge, this gives agencies a fighting chance to succeed with HHVBP. Data drives decisions. Great data drives great decisions. Knowledge is power. That can lead to a 5% raise, or at worst staying even.
By proactively approaching the upcoming changes, agencies set themselves up for success going into 2025 and the very real challenges they face. Ask us how we can help- and optimize coding and OASIS for accuracy and financial success. Agencies can actually thrive in this environment and be rewarded for outperforming their peers.